Every Operating Room case has an average of 4 conflicts. Those conflicts have the potential to affect safety , patient care and efficiency.
This paper, which collected conflict stories from operating room personnel in a Swiss teaching hospital, found that 4 out of ten of the episodes of conflict experienced by OR staff had an impact on providing timely, patient-centered and efficient care.
There are several aspects of this study which are worth noting.
The paper discussed the direct and indirect effects of conflict in the patient care realm. Direct effects of conflict relate to patient care delays and the quality of care. Indirect effects include the mental distraction of staff from clinical duties and impact on their mental health. Conflict during work hours can directly contribute to burnout.
Surveyed participants were classified by teams with the same specialty or job (intraprofessional) , different specialty or job (interprofessional) and by hierarchy (nurse manager/ nurse, chief resident/ resident). Patient-centered consequences were more associated with intraprofessional conflicts. Interprofessional conflicts, in which different groups or specialties may be in disagreement, would be more likely to result in delay of care.
The conflict stories were coded and the participants were asked to comment on whether they felt that the conflict impacted patient safety. The six dimensions of quality cited by the Institute of Medicine, timeliness, patient-centeredness, efficiency, effectiveness, safety and equity were used. The most common associated outcomes of conflict cited were failure to provide timely, patient-centered, and less efficient care.
This paper suggests that, in assessing Operating Room efficiency, conflict must be considered and assessed. Use of semistructured interviews is a powerful tool to assess the presence of conflict in the perioperative setting. These stories can be coded and stratified to assess intraprofessional, interprofessional and hierarchical conflict.
Conflict, once recognized and assessed, serves as a platform to improve efficiency, patient care, and the mental health of all staff. Strategies for conflict recognition and processing can be employed.
I remember the first robotic surgical procedure I participated in after the Covid 19 lockdown began in March of 2020. I read articles and followed Facebook groups of doctors practicing in high volume areas, primarily New York. Many of the procedures followed were gleaned directly from their advice and experience. They were the front line. One hospital in particular, Elmhurst in the Bronx, was considered “the epicenter of the epicenter”. This hospital, which is in the Mount Sinai system, has resident physicians who are primarily foreign medical graduates caring for a very diverse community.
At the end of May 2023, these resident physicians, as part of the Committee of Interns and Residents/Service Employees International Union, went on strike.
Among the many articles about the strike, in which the residents cited a lack of pay parity with other residents in the Mount Sinai health care system, but also a lack of support and recognition for the tremendous amount of work and emotional effort required during one of the darkest periods in the history of the world’s health care systems.
The resident physicians, in negotiations with Mount Sinai, repeatedly made demands for workforce support, which included pay commensurate with other residents in the Mount Sinai hospital system. In a statement released to the residents by the hospital administration, a chart with the proposed salary increases includes this statement ; “there was very little response to our generous package proposal” (1).
Ultimately, after a three-day strike, residents from specialties in Internal Medicine, Psychiatry and Pediatrics went back to work with a negotiated salary much closer to that of their other peers in New York.
In a statement from the Committee of Interns and Residents, Dr. Sarah Hafuth said “This fight was always about power, and Elmhurst residents are truly building that together”. (2)
In a sense, the Mount Sinai H + H system was bringing a knife to a gunfight.
The experience of those of us in healthcare during the pandemic was the product of an already stressed and dysfunctional system pressed to an untenable extreme. Having worked in hospitals since my first job almost forty years ago, I honestly have never witnessed the helplessness, fear, frustration and anger that was so palpable during the pandemic. We struggled collectively to put a word to the cloud that surrounded and suffocated us. It does have a name.
Moral Injury.
Moral injury can occur when someone engages in, fails to prevent, or witnesses acts that conflict with their values or beliefs. Examples of events that may lead to moral injury include:
Having to make decisions that affect the survival of others or where all options will lead to a negative outcome
Doing something that goes against your beliefs (referred to as an act of commission)
Failing to do something in line with your beliefs (referred to as an act of omission)
Witnessing or learning about such an act
Experiencing betrayal by trusted others
Watson et al, “Moral Injury in Health Care Workers” PTSD:National Center for PTSD
A strike is a conflict in which the parties have engaged in collective bargaining, but have been unable to effect resolution through negotiation. It is the final common pathway for a party unwilling or unable to accept the proposed solution. In conflict management, one of the most common reasons for the inability of the involved parties to reach a solution is that one or both parties are unaware of the reason or reasons for the conflict
In reading the Mount Sinai H + H statement, there is no mention of the moral injury, either by name or by the unbelievable situations in which the student doctors found themselves. The offer includes increased pay for a Chief Resident, six week paid leave of absence, expanding medical education benefits, and “creating language” for hazard pay (not guaranteeing hazard pay itself). These are interest based solutions. Interest based solutions are quantifiable. It is easy, on some level, to argue about the number of apples you are going to give me. It’s just a number. And while we might disagree on the number, for the person offering the apples, there is much less effort involved in figuring out how many apples are required to make me go away and leave you alone.
But let’s say the apples represent far more to me than just a number. I remember when there were no apples. I remember that even if there were apples available, I didn’t have ladders to get apples for the people who needed them. When people who were my responsibility didn’t get apples, they suffered greatly. At times, I had to decide who got apples and who didn’t. Those memories don’t go away. My worldview of apples changes. Until this is addressed, there will be no resolution to the conflict.
“So, think of me as any particular employee. If I work for your company, you have expectations. You expect me to come to work. You expect me to be there on time. You expect me to do my job well to the best of my ability. I also have expectations. I expect to be provided with the tools to do my work from a moral standpoint. So, if I come to work and my employer does not supply me with what I need, I am injured morally. When my employer doesn’t supply me with enough colleagues to distribute the workload or PPE for my protection—the gowns, masks, face shields, and gloves I need—that is both insult and injury to me. My employer is not standing by the employment contract; both sides have an expectation, but one side is letting the other side down. This results in psychological harm to one’s belief system.”
Alexis Rean-Walker, Nurse, HPAE (4)
Dr. Suzanne Shale describes moral injury related to the Covid 19 pandemic (6). She describes the circumstances that lead to moral injury related to the pandemic, experienced by patients and family within the health care system as well as providers. In her words, “moral injury requires moral repair”. She lists seven ways institutions can begin to address moral repair.
Acknowledge the injured party is a moral equal.
In a statement from the CIR, it is stated that the Elmhurst strike was about “power”. This is consistent with moral injury. Interest based conflict would have been easily resolved just by increasing reimbursement of the striking physicians to a level commensurate with their peers. To truly resolve the conflict, the hospital should offer residents a voice to directly contribute to hospital policy and management. For example, inviting house staff to have regular, valued input with hospital administration with documented effort at adoption would be a sign of equality.
Acknowledge the authority of shared norms.
The guiding principle of placing patient care as the primary
of any health care system is the very definition of a shared norm.
Violation of that norm was clearly exhibited both during and after the pandemic. It persists as evidenced by the lack of provision of staff and infrastructure to meet the standard of care.
It is not possible to say that you place patient care and safety as a first priority while having one nurse care for eight patients (or more) on the floor. Keeping a resident on shift longer than twenty-four hours because there are no attending physicians available increases the risk of error on the part of the well-meaning but exhausted doctor. When healthcare workers strike in the name of better patient care, this is sincere. They have seen, with their own eyes, the struggle to provide the best care they can with the most meager resources available. However, when hospital administrators state repeatedly that money is the primary issue, one suspects that money is the primary issue FOR THEM. Because both parties have different norms and motivations, conflict persists.
Acknowledging injury.
There must be a context and an opportunity to speak of the
harms of that occurred and give them voice and legitimacy. Administrators responsible for keeping hospitals open during the pandemic have no doubt experienced stress and harm also. Stories shared on social media and within groups, while producing resonance, are not the same as having the profound trauma recognized by those perceived to be in leadership. “Lip service” given to this, which may occur by making short references to the injury, may almost work in the opposite way. The recognition of the injury becomes a bullet point instead of a significant part of what is required to heal.
This should be a formal process, whether by in-person meetings, town halls, or shared written documentation. To speak of the injury creates a real and living acknowledgement, and takes a public and definite step toward repair.
Acknowledging responsibility.
Dr. Shale states in her article that acknowledging responsibility is not the same as assigning blame. It is a person or institution recognizing that a part was played by them in the occurrence of moral injury. Because of this, it is paramount to accept a role in the process of reconciliation.
The pandemic was not the fault of the health care system at large, or the administrators and non-clinical staff. They were working in impossible situations. The already fragile infrastructure of the American hospital system was stressed to its maximum and beyond during the height of COVID. As thousands of health care providers, including nurses, doctors, and staff stopped working after COVID, the numbers of personnel available to meet the needs of patients surging back into the system for outpatient care and preventive medicine were not available.
Those continuing to work found themselves overloaded, and those in the non-clinical hierarchy did not take active accountability for this.
Financial reward does not meet the need or repair the deep emotional trauma of being taken for granted. If the assumption is that there will always be someone available to work a shift, do a procedure, or write a prescription, there will never be the acknowledgement of the systemic failure which continues to affect the work life of those in health care, and indirectly the life of the patient.
Acknowledging that remedy is due.
This may be the most challenging of all. To admit that moral injury occurred, by definition, means that it must be repaired. This is also why moral injury must be defined and recognized as a separate entity from burnout.
Burnout by definition is localized to the individual; “exhaustion of physical or emotional strength or motivation usually as a result of prolonged stress or frustration” (7). If we define the experience of the striking individual as being “burned out”, it is simple (and easier) to assign solutions which address the individual in ways suited to this definition. I heard one operating room employee say that when they reported how significantly short-staffed and exhausted they were, hospital administration listened, then bought them pizza the next day. Nothing else was done. Now, when there are staffing issues to the point that employees are not given breaks to eat, they simply say there is no point in saying anything. “They will just say ‘sorry’ and buy pizza”.
Moral injury is a systemic issue. It occurs when the individual encounters that the system which was supposed to keep their interests first and share their values and norms has betrayed them. Because it is systemic in nature, efforts directed to the individual such as time off, wellness programs, and other more easily quantifiable measures are much less likely to resolve concerns or provide remedy. It is also much more difficult to heal systemic issues.
The failure to offer remedy may also serve as a “second harm’. Once the moral injury has occurred, for the system to fail to acknowledge that remedy is due may actually compound the moral injury itself. If hospitals try to ignore systemic solutions which legitimately would provide healing to providers and better care to patients, either because those solutions seem too difficult or because it may be easier to address them as purely financial, moral injury will persist and work stoppage will be much more common.
Acknowledging righteous anger, or other negative feelings.
Witnessing the healthcare environment of the pandemic is something I will never forget. The fear of going to work every day and not knowing if you would bring COVID home to children and family. My husband is a pulmonologist and we decided early into the COVID outbreak that we would not sleep in separate rooms, If one of us got COVID, we likely both would. I remember every day waking up and worrying if I lost my sense of smell, and keeping a jar of garlic in the fridge just so I could make sure I could sniff it. As a physician in solo practice, I didn’t know what would happen if I contracted COVID and was unable to care for patients or pay my employees.
As many negative feelings as I have, I cannot fathom the inerasable memories of my friends and colleagues. Those who watched countless people die, helpless to save them. To simply put these feelings away and get back to work is not tenable. Those providing patient care in hospital systems need TIME. The ability for administration to provide understanding and space only can occur when providers are viewed as individuals who have been morally injured, and not resources within the hospital infrastructure.
Indeed, to see people as being morally injured and create the space to recover is a litmus test. If this occurs, it is a sign that the system is moving away from seeing people as individuals and not as necessary cogs in a machine.
Acknowledging that, in injuring each other, we should experience sorrow and regret.
There is no price tag on sorrow. More than anything, this expresses why money alone will not stop resident strikes. The lack of genuine remorse for what these residents at Elmhurst have been through is palpably absent in the written statement released by Mount Sinai. If anything, painting these house officers as being driven by money alone ignores the very soul of moral injury that they have experienced. I would hope there would be a moment of meeting, a time in which hands could be held and those in administration could cry with the residents and say “I am so sorry you had to have this experience so early in your career”.
This kind of love and support is the very thing required to begin the healing process.
Until the disease causing the strikes is correctly diagnosed, it will persist. It must be called by its name. Moral Injury. Until this occurs, the strikes will continue.
I hope that recognition on the part of those in leadership in the healthcare system will occur quickly.
Ulrich, C. M. and C. Grady. 2019. Moral Distress and Moral Strength Among Clinicians in Health Care Systems: A Call for Research. NAM Perspectives. Commentary, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201909c
6.
Shale SMoral injury and the COVID-19 pandemic: reframing what it is, who it affects and how care leaders can manage itBMJ Leader 2020;4:224-227.
We make diagnoses. We deliver babies. We take out inflamed appendices. We treat depression, lower blood pressure, and manage urinary tract infections. In dark rooms and under microscopes, we exercise our intellect. Whether we are teachers, learners, or consultants, we exercise our art.
We are more.
More than the white coats we wear. More than a set of data for pharmaceutical companies. More than a source of income for health care systems.
We hold the hands of our patients, as well as our staff and colleagues. We work ourselves to exhaustion at times, just because we know we are needed. Even though we are not always ready, we make ourselves readily available.
In the last 18 months, I have seen more heroism in the real life of clinical medicine than I have seen in any Marvel movie.
I know, without a doubt, we are more.
We help colleagues grow practices and recruit new staff. We refer patients to them, because we know they will receive quality care.
Routinely, we check on our friends in practice, making sure they are caring for themselves. We ask the real questions. Instead of asking “how are you”, asking “when are we having pizza and a movie?”
We are those who are mindful of the emotional and physical drains of this life, knowing that the supporting hug is a greater blessing than the accusing finger.
In preparation for the current blog series, I have spend a decent amount of time researching the concept of uncertainty in medical decision making. Several articles have jumped out, some of which I will be posting. This idea of becoming more comfortable with being unsure about diagnoses and the practice of medicine has in many ways been therapeutic, maybe even more so than being a professional and intellectual question. I know I am not comfortable with not knowing. In my heart, I have always been concerned that, if I expressed my uncertainty, I would be judged and belittled.
It was a source of comfort, then, to find so many articles in which others felt the same way. It is easy to isolate ourselves in busy schedules; creating the space to be vulnerable with a person we trust is a great luxury. It is not always readily available.
One of the emails I get almost every day is from the Center for Action and Contemplation, a site devoted to the meditative practices of Christianity. Richard Rohr, whose writings are on the blog, speaks in such a way that I wonder how he knows exactly what I need to hear on any given day. Today was no exception.
It’s a short read that almost begs to be re-read and digested.
The post today was about uncertainty in a spiritual sense. One of the things Rohr talks about is the natural path from faith to doubt, and back to faith again with the knowledge that our faith rests in the Divine, not in the apparent “reality” we perceive. The questioning, that space of uncertainty, takes us to a stronger place. Even if it doesn’t feel good at the time.
“What has happened to our ability to dwell in unknowing, to live inside a question and coexist with the tensions of uncertainty? Where is our willingness to incubate pain and let it birth something new? What has happened to patient unfolding, to endurance? These things are what form the ground of waiting. And if you look carefully, you’ll see that they’re also the seedbed of creativity and growth—what allows us to do the daring and to break through to newness. . . .
Creativity flourishes not in certainty but in questions. Growth germinates not in tent dwelling but in upheaval. Yet the seduction is always security rather than venturing, instant knowing rather than deliberate waiting. “ – Sue Monk Kidd
Wow. That last line.
Actively venturing into the space of uncertainty is a necessity, just by virtue of the art we practice. We can never know it all, yet deliberately wading into the sea of what we have yet to learn for the benefit of those we serve is at the core of what makes us effective as health care professionals.
Thank you for reading. Peace.
Sue Monk Kidd, When the Heart Waits: Spiritual Direction for Life’s Sacred Questions (HarperSanFrancisco: 1990), 25.
Richard Rohr, Falling Upward: A Spirituality for the Two Halves of Life (Jossey-Bass: 2011), 111‒113; and
Richard Rohr, The Naked Now: Learning to See as the Mystics See (The Crossroad Publishing Company: 2009), 117.
This link below is to an article posted in the Lancet online Psychiatry posted last week regarding medical diagnosis and uncertainty in the face of Covid-19.
Health professionals sat down in pairs to discuss their response to the currrent health crisis. They were recorded, with names scrubbed for anonymity. Two things were observed. The first was the pervading sense of uncertainty about how to proceed and care for patients during this pandemic; the second was that there was no one to talk to about the first. The article recommends the following as a course of progress.
“Charting a course of action in the face of uncertainty—an uncertainty that sows doubt about one’s own professional role and value—is not simply a matter of having access to information. It requires being psychologically ready and able to bear that feeling to determine what best can be done, even when knowledge is restricted. Achieving this readiness requires that the doctor (or nurse) recognises that they are not alone—they are part of a community of peers. A community in which they can, privately and securely, express concerns about feeling ineffective, powerless, and isolated—enervating states often associated with shame. In other words, managing uncertainty is rooted in two requisites: first, a state of mind able to bear uncertainty, yet still act; and second, knowledge, which in this case was at first too scarce and then only incrementally expanded. Not attending to the former requisite arrests entry into the latter.”
I love this. Mainly because I think I have had this feeling so often, and yet never had the courage to talk about it (except to my husband, a pulmonologist. Poor guy. He’s probably really happy I have this blog so I don’t subject him to my mental meanderings). “[A] state of mind able to bear uncertainty, yet still act”.
For us, accepting the state of being uncertain, having the strength to admit it to our peers, and allowing it to be a gateway into a greater state of information and wisdom is not only beneficial to our patients. It is essential to our well-being as clinicians.
Before I go, if you want to gauge your tolerance of uncertainty as we go into this week, here is a quick little internet quiz.
“Medicine is a science of uncertainty and an art of probability”
-Sir William Osler
There were many people who were saddened at the passing of Alex Trebek. My family was no exception. My parents and I would watch “Jeopardy!” At 6 pm, yelling out answers while eating dinner. Without fail we would yell at the players to bet it all on the Daily Double; my mom and dad would marvel at how I could miss most of the questions in the History section and yet run the category on Potent Potables. Decades later, I still watch it with my family. And I always feel a little bad when I miss a question.
Alex’s fellow Canadian Dr. Osler, one of the founders of Johns Hopkins Hospital and a renowned diagnostician, probably would have rocked “Jeopardy!”. Interesting, given his quote above. Are we, as a profession, comfortable with being uncertain?
“Tolerating Uncertainty- the Next Medical Revolution?” , link below, was published in the NEJM in 2016. It’s only two pages and totally worth the read.
It really doesn’t even question whether or not we as medical professionals are comfortable with uncertainty. It just assumes we aren’t. We are constantly presented during the educational process with messsages that we are either “right” or “stupid”.
Uncertainty=ignorance
In our minds, the path to success begins with the correct answer. Anything else is unacceptable. The jump to a diagnosis to just to get to an answer may be just as problematic, as we may miss key information or exercise cognitive bias for no other reason than we want to push that button and get our Daily Double correct.
Trying to achieve a sense of certainty too quickly
|
| < cognitive bias
|
Premature closure of the decision making process.
Ok. So how to make this process change? The authors suggest that the first thing to do is to not equate uncertainty with a lack of knowledge or being bad at what we do. Uncertainty is not the final destination. It’s a rest stop. If uncertainty is the rest stop, then what’s the car we drive to get there?
Tolerance of uncertainty ——> CURIOSITY
Wanting to know the answer, being transparent about not knowing the answer and committing to the patient that we truly desire to get to it for their benefit. Maybe that’s why the authors equate a decreasing ability to tolerate being uncertain with an increased risk of burnout. The pressure to be “right” all the time is not realistic.
I teach martial arts in my spare time (it’s therapy for me. Anti-burnout meds. And to spar kids half my age and not get beat up bolsters my ego) and we traditionally ask students questions at belt rank exams about martial arts history, techniques, etc. We do our best as instructors to teach students the information they need for this, but of course sometimes they freeze up at testing. So we teach them one simple phrase if they forget.
“I don’t know, but I will find out”.
We teach them that that is a perfectly acceptable answer. AND IT IS. We are not taught to do this in medical school or residency. And we don’t realize that, when we say this to our patient, because we really don’t know and we need to take more history, do another physical, do more research, maybe do another test, that the patient is absolutely fine with it. In my experience, patients are much more likely to have a collaborative relationship with a physician who honestly expresses his or her humanity.
It’s not about right or wrong. Maybe the best bit of evidence that lets us know that’s it is ok ?
I want to be a Jedi.
Next up. Is there a way to assess our natural tolerance of uncertainty?
Anyone who reads medical literature on the regular has seen “p” values. We have a basic understanding of the statistics used (I’m totally referring to myself; I have relearned statistics in a short-term form for almost every board exam I’ve ever taken).
It wasn’t until I started the deep dive into medical diagnosis and the fits and foibles thereof that I learned about Bayes theorem.
Basically, the frequentist says “common things are common”. “When you hear hoofbeats, think horses”.
The Bayesian says, “ I hear hoofbeats. It must be horses”, but then looks out the window and says “but I see black and white stripes on those horses. Sooo, maybe those hoofbeats are zebras”. Bayesians update the hypothesis based on the new data collected.
I wonder if there are many truly excellent diagnosticians out there who are Bayesians, and don’t even know it.
I also wonder how often we miss the diagnosis in front of us because of frequentism.
Thanks for reading and considering. More to come. Peace.
In my experience, transparency is not something discussed with regard to clinical decision making. This is a link posted by the Patient and Client Council, to promote a project from the Clinical Education Center in Northern Ireland. They are asking for patients to participate in a Zoom conference to discuss Shared Decision Making between patients and clinicians.
“Shared decision making is a process in which individuals and clinicians work together to understand and decide what tests, treatments, or support packages are most suitable bearing in mind a person’s own circumstances. It brings together the individual’s expertise about themselves and what is important to them together with the clinician’s knowledge about the benefits and risks of the options”.
My dad had a great saying for his medical students and residents.
“Eighty percent of the patients we see will get better no matter what we do, 10 percent will get worse no matter what we do. It’s the ten percent in between that we have a true opportunity to help”.
And his students probably never said this to him, but I was his daughter. I could get away with it
“Dad, how do we know which is the ten percent we can help?”
How do we identify those patients? And even if we could do that, how do we make sure we don’t screw it up and miss something?
This one concept leads us most readily into the importance of understanding the diagnostic process, and ourselves within it; the cognitive nature of medical diagnosis, even within the larger framework of decision making as a whole.
We could actually go through each chart in which a diagnosis is missed, reviewing the clinician’s process, looking at the data and deciding where the breakdown in decision making occurred. There are LOTS of problems with this.
It’s a hard-fought [sporting event of your choice] and we already know who won and lost. Knowing the end absolutely skews data analysis. We are looking for confirmation of a diagnosis in which we are confident is correct.
Because we know the end, small pieces of information which would have been central to making the diagnosis are more easily recognized. The narrative changes because we are telling the story with the documented conclusion in mind.
We have oodles and oodles of time to review a chart. The clinician had maybe 5 minutes to see the patient and review the data. We are looking at the chart at our comfy desk with a cup of pour-over and fuzzy socks. The guy or girl who did the work was seeing upwards of thirty patients in clinic and was trying to get to his or her kid’s soccer game at 530.
Chances are, if a chart is being reviewed, something bad happened. While we all seek to be excellent diagnosticians, The main reason this whole topic even matters is because we are trying to avoid the catastrophic outcome.
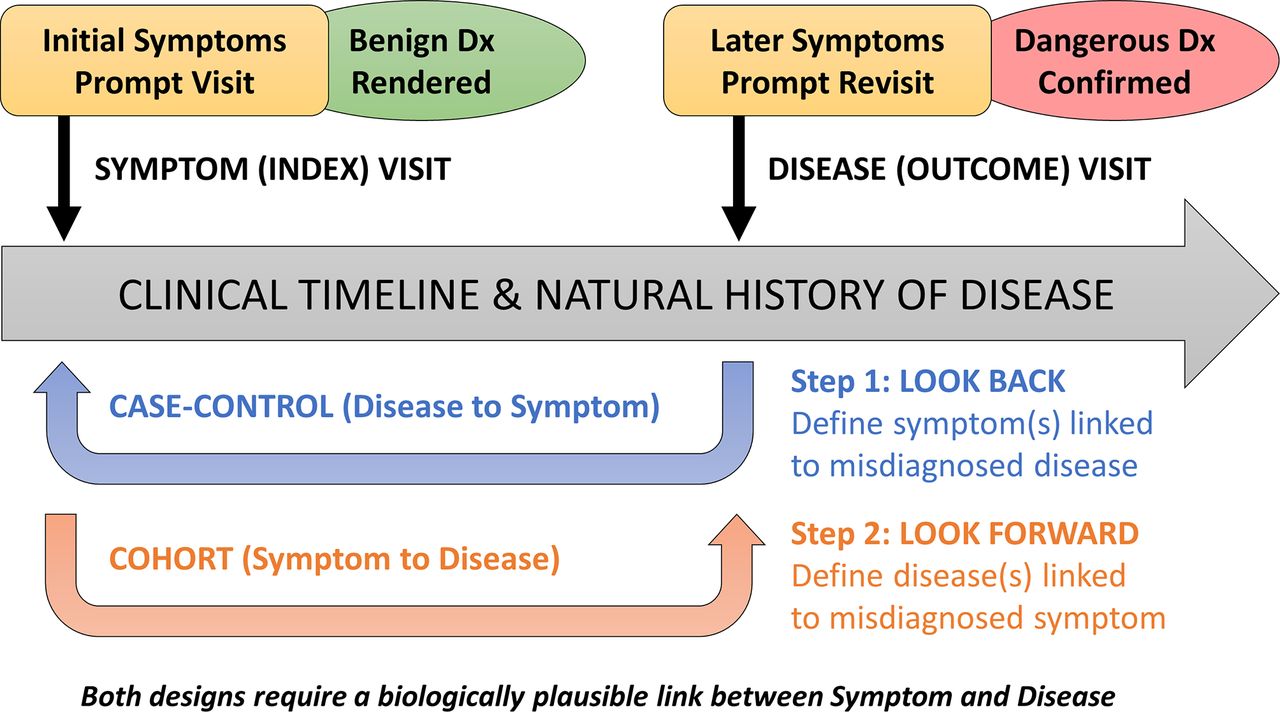
A paper published in the British Medical Journal in 2018 sought to take a broader scope of data review to identify problems with medical decision making. It discussed using Symptom- Disease Pair Analysis of Diagnostic Error (SPADE) to look at large blocks of clinical data and identify missed diagnoses (Lieberman and Newman-Toker, 2018)
Let’s say you have a 25 year old otherwise healthy female patient that comes in to an urgent care with shortness of breath. The patient is worked up, and the physician who sees her diagnoses her with bronchitis, gives her antibiotics and sends her home. Two days later, the patient presents to the Emergency Department, bottle of antibiotics in hand, with significant worsening of her symptoms. At that time, she undergoes a VQ scan which is read as high probability and she is diagnosed with a pulmonary embolus . On review of her records, we find she was started on combination oral contraceptives in the last three months, which increased her risk of thrombotic events. She is started on anticoagulants, changed to a progestin- only oral contraceptive, and is discharged home in good condition.
In our SPADE analysis, we would use the symptom-disease pair of shortness of breath- pulmonary embolus.
“The framework shown here illustrates differences in structure and goals of the ‘look back’ (disease to symptoms) and ‘look forward’ (symptoms to disease) analytical pathways. These pathways can be thought of as a deliberate sequence that begins with a target disease known to cause poor patient outcomes when a diagnostic error occurs: (1) the ‘look back’ approach defines the spectrum of high-risk presenting symptoms for which the target disease is likely to be missed or misdiagnosed; (2) the ‘look forward’ approach defines the frequency of diseases missed or misdiagnosed for a given high-risk symptom presentation.” (Lieberman and Newman-Toker, 2018) .
Ideally, we can collect SPADE data on a multiplicity of symptom-diagnosis dyads and look at the number of times a diagnosis is missed by “looking back”. We can then use that data to “look forward”, based on a patient’s symptom presentation.
The authors point out that because of the ease is identifying symptoms and diagnoses in different health system databases (ICD-10 might be our friend after all:)) that collecting large amounts of data and calculating frequency of symptom to diagnosis should not only show us how often miss, it should allow us to see when we improve.
Cool. “Cool cool cool”. (Abed, “Community” 2009).
But wait. If SPADE can show us symptom-diagnosis dyads, indicating the frequency which they two may be associated, is it possible to calculate the likelihood of having a disease given a presenting symptom? And if so, are there other associated factors which may make the disease more likely in the presence of said symptom (i.e. new start oral contraceptive use and pulmonary emboli) ?
Stay tuned. We are just getting started on our journey. Thanks for reading. Peace.
“Pilot”.Community . Season 1, Episode 1, NBC, September 17,2009.
Liberman AL, Newman-Toker DE Symptom-Disease Pair Analysis of Diagnostic Error (SPADE): a conceptual framework and methodological approach for unearthing misdiagnosis-related harms using big data BMJ Quality & Safety 2018;27:557-566.




{kind=link}